
An enlarged prostate is one of the most common conditions affecting men over 50, and the urinary symptoms it causes – the weak stream, the trips to the bathroom at 2am, the sensation of never quite finishing – affect quality of life in ways that are easy to underestimate until they’ve been going on for years. Most men adapt gradually to worsening symptoms and assume either that nothing can be done or that the only options involve surgery with significant recovery and side effects. Neither assumption holds up. At Lazare Urology in Brooklyn, BPH evaluation and treatment is a central part of the practice, and the range of options available now – including UroLift, which can be performed in an in-office setting under sedation – is considerably wider than what many men realize.
Understanding the condition, the treatment options, and how they compare is the starting point for making a decision that fits the specific pattern of symptoms and priorities.
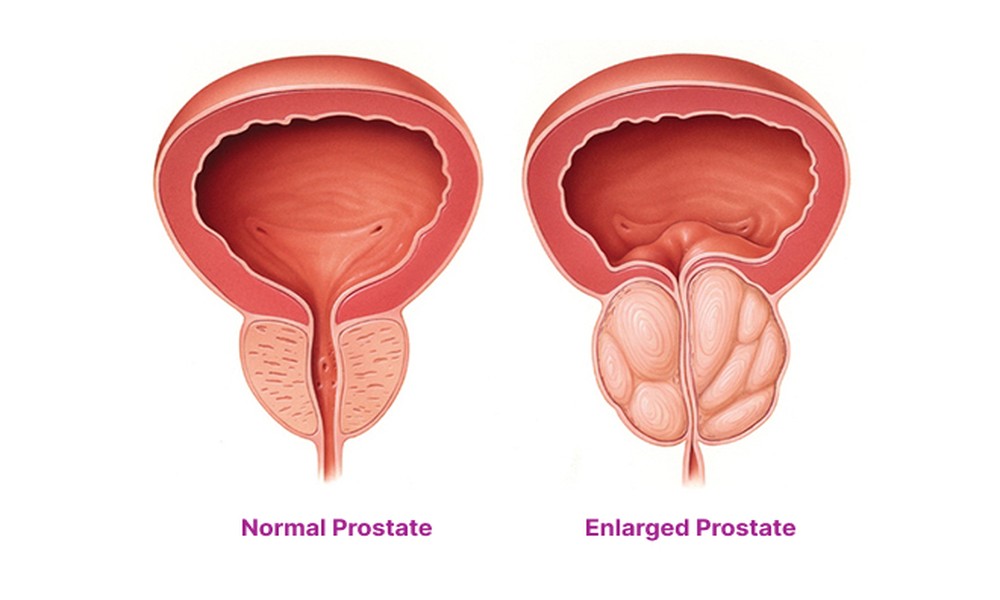
What BPH Is and Why the Prostate Causes Urinary Symptoms
Benign prostatic hyperplasia is the non-cancerous enlargement of the prostate gland that occurs with age. The prostate surrounds the urethra just below the bladder. As it grows, it compresses the urethral channel, obstructing urinary flow to varying degrees. This is a mechanical problem – the gland itself is benign, and BPH is not a precursor to or risk factor for prostate cancer, though both can coexist.
The symptoms that BPH produces fall into two overlapping categories. Obstructive symptoms result directly from urethral compression: a weak or intermittent urinary stream, straining to initiate urination, prolonged voiding time, and a sense of incomplete bladder emptying that prompts a return to the bathroom shortly after urinating. Irritative symptoms reflect the bladder’s response to obstruction over time: increased urinary frequency, urgency, and nocturia – the nighttime awakening that many BPH patients find most disruptive to their daily lives.
The International Prostate Symptom Score (IPSS) is the standardized questionnaire urologists use to quantify BPH symptom severity, and it helps track both baseline severity and response to treatment. A score in the mild range suggests monitoring may be appropriate; moderate to severe scores generally indicate that treatment deserves serious consideration.
When Watchful Waiting Is Appropriate
Not every man with BPH symptoms needs immediate intervention. Watchful waiting, combined with behavioral modifications, is a reasonable approach for men with mild symptoms whose quality of life is not significantly affected.
Behavioral modifications that can reduce symptom burden include limiting fluid intake in the hours before bedtime, reducing caffeine and alcohol (both of which have diuretic effects and can irritate the bladder), timed voiding, and double-voiding (urinating, waiting a few minutes, then attempting to urinate again to more fully empty the bladder). These measures don’t treat the underlying enlargement, but they can reduce the functional impact of the obstruction sufficiently that active treatment isn’t immediately necessary.
The appropriate time to move from watchful waiting to treatment is when symptoms are moderate to severe on the IPSS, when urinary retention has occurred, when the bladder is not emptying adequately enough to be measured as significant post-void residual, or when the impact on sleep and daily function has become unacceptable to the patient. The threshold is in part clinical and in part a matter of what the patient finds tolerable. A man who has adapted to getting up twice a night and is otherwise not bothered has a different situation than a man who is getting up four times, is sleep-deprived, and is limiting his activities to stay near a bathroom.
Medications: What They Do and Where They Fall Short
Alpha-blockers – tamsulosin (Flomax), alfuzosin, silodosin – are the most commonly prescribed first-line medications for BPH. They work by relaxing the smooth muscle in the prostate and bladder neck, reducing urethral resistance without affecting the size of the gland. They are effective for improving urinary flow and reducing obstructive symptoms in many men, typically within a few weeks of starting. Side effects include dizziness, particularly orthostatic hypotension, and retrograde ejaculation, which is common with some agents in this class.
5-alpha-reductase inhibitors – finasteride and dutasteride – work by reducing DHT, the androgen that drives prostate enlargement. Unlike alpha-blockers, they actually shrink the prostate over time, typically by 20-30% over 3-6 months. They are most effective in men with significantly enlarged glands and are often used in combination with alpha-blockers. Sexual side effects – decreased libido, ejaculatory dysfunction, and less commonly erectile dysfunction – affect a subset of men on these medications.
The limitation of medications as a long-term strategy is that they manage symptoms without correcting the mechanical obstruction. Men on alpha-blockers often need to continue indefinitely; stopping the medication typically results in symptoms returning. Men whose symptoms progress despite medications eventually reach the point where procedural intervention provides a more durable solution.
How UroLift Works and Who Is an Appropriate Candidate
UroLift is a minimally invasive procedure that addresses BPH through mechanical tissue retraction rather than tissue removal or ablation. Small implants are delivered through a cystoscope and anchor the enlarged prostatic lobes in a retracted position, opening the urethral channel without cutting, heating, or removing tissue.
The procedure does not destroy prostate tissue. It physically moves the obstructing tissue out of the urethral pathway and holds it there with permanent implants. The result is improved urinary flow without the tissue removal required by TURP or the thermal injury involved in laser procedures.
The candidate profile for UroLift is specific. The procedure is most effective in men with lateral lobe enlargement – the pattern in which the prostate lobes compress the urethra from the sides. Men with a significantly enlarged middle lobe that protrudes directly into the bladder are not ideal candidates, because the UroLift implants address lateral tissue rather than the intravesical component. Prostate size also affects candidacy, with optimal results in glands below a certain volume threshold; very large prostates may be better served by other approaches.
The significant advantage of UroLift relative to TURP and laser procedures is the sexual side effect profile. TURP carries a high rate of retrograde ejaculation – typically reported at 65-90% – which is permanent. UroLift data shows preservation of sexual function, including ejaculation, in the large majority of men who undergo the procedure. For men who place significant value on preserving ejaculatory function, this is a meaningful consideration in the choice between procedures.
UroLift at Lazare Urology: The In-Office Sedation Setting
UroLift at Lazare Urology is performed in the certified in-office operating room with IV sedation administered by a board-certified anesthesiologist. The procedure itself is delivered through a cystoscope and takes approximately 30-60 minutes. Being sedated rather than simply given local or topical anesthetic means the patient is not aware during the procedure, which involves passage of the cystoscope and deployment of the implants – an experience that, under sedation, the patient does not experience at all.
Recovery after UroLift is markedly different from TURP. Most men experience temporary urinary symptoms for one to two weeks as the tissue responds to the implants – some urgency, frequency, or discomfort – before these resolve and urinary flow improvement becomes apparent. Catheter use is not required in most cases, or is short-term. Most men return to normal activity within a few days. Improvement in urinary symptoms is typically evident within two to four weeks.
TURP, by comparison, requires hospital admission, carries a longer recovery, and typically involves a catheter for several days post-procedure. It removes tissue through electrosurgical resection, which is effective for large glands but involves more recovery burden.
Making the Right Decision for Your Specific Situation With Lazare Urology
There is no single right answer for BPH treatment that applies to all men. The appropriate option depends on symptom severity, prostate size and anatomy, the degree to which sexual side effects are a priority, overall health, and how much disruption the patient is currently experiencing and willing to accept in a recovery period.
Lazare Urology in Brooklyn evaluates men with BPH symptoms with a complete assessment – including IPSS scoring, post-void residual measurement, and anatomical evaluation – to determine which treatment approach fits the individual patient. Contact the office to schedule a consultation and get a clear picture of what your options are and which one serves your situation.